
Dr. Pandher
Orthopaedic Surgeon

ACL, PCL & Meniscus
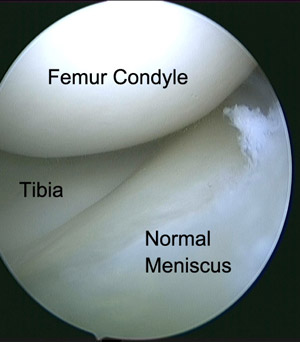
ACL & PCL are the major struts of the knee joint which prevent the tibia (leg bone) form sliding anteriorly or posteriorly on the femur (thigh bone). These ligaments can be damaged in sports injury, road traffic accident or even domestic fall. Patient generally complains of knee giving away or twisting out. If this issue is not addressed urgently, repeated abnormal movement at the knee joint leads to further damage to the supporting structures of the knee joint. For this reason patients presenting late often have complex meniscal tears and cartilage damage.
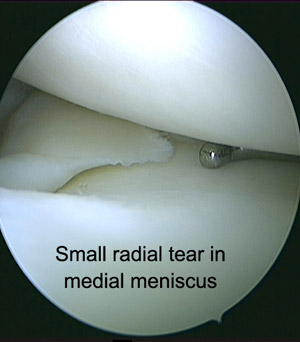
Since ACL is the most commonly injured ligament in the knee we will discuss it in detail. Meniscus injury is often associated with ACL tears and is always addressed along with ACL reconstruction surgery. There are two treatment options available for meniscus injury. If the tear is around the periphery of meniscus and its structure is not badly damaged, we favor to repair the torn meniscus. However, players often present late with advanced damage to the meniscus where only treatment option viable is to remove (excise) the torn part of meniscus.
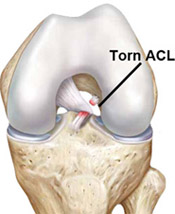
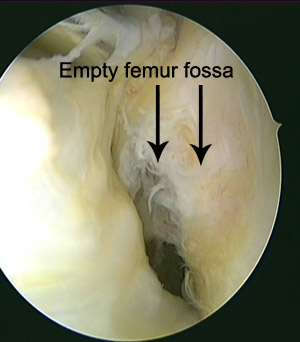
ACL is the abbreviation for the Anterior Cruciate Ligament. This is one of the major stabilising ligaments within the knee. It connects the thigh bone (femur) to the leg bone (tibia) and prevents abnormal movement (instability) occurring between the two. More specifically it provides rotatory stability to the knee to allow movements such as pivoting or sudden change in direction to occur without the knee giving way.
The most common mechanism of injury is from a non-contact injury that typically occurs whilst attempting a pivoting or cutting (change of direction) maneuver whilst playing sport.
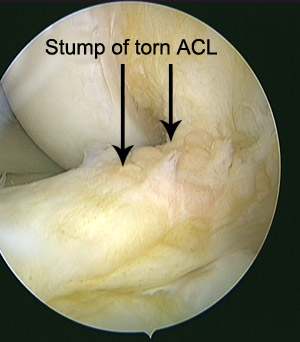
The injury can also occur from contact activity (e.g. being tackled from the side) when your knee buckles inwards whilst the leg is held in a fixed position. Not uncommonly, a “cracking or popping” sensation is felt at the time of the injury. The injury is associated with a lot of swelling within the knee that typically occurs at the time of, or soon after the injury. The leg is often painful to walk on for several days.

An ACL rupture may be associated with an injury to other stabilizing ligaments within the knee. Rupture of your ACL is commonly associated with tears that involve the shock absorbing cartilages (menisci) of the knee. Depending on the location and size of these tears they may be surgically repaired or excised at the time of your surgery. Bruising of the bone also occurs at the time of injury because your thigh and leg bones are driven into each other by the violent forces that cause the ligament to rupture. No specific treatment is required for this "bone bruising".
If your knee is giving way regularly and this is interfering with your quality of life, you may want to consider an operation. This instability may occur during sport or during activities of daily living. Most patients who want to return to pivoting sports will require a reconstruction to prevent their knee buckling during these activities.
An ACL reconstruction is not an urgent or emergency operation. Your knee has suffered a lot of damage at the time of injury, and the best outcome from reconstructive surgery has been shown to occur in people whose knees have had some time to stabilize and recover. In the majority of cases we prefer to rehabilitate your knee prior to undergoing surgery. This involves controlling the swelling, regaining the movement in the knee and preventing or limiting the loss of strength in the muscles around your knee. This period of rehabilitation can take from 7 days to 6 weeks. Performing physiotherapy before your surgery also teaches you the exercises needed for rehabilitation after the surgery. The majority of patients who have an ACL rupture are unable to return to pivoting or cutting sports without experiencing instability (especially if performing at an “elite” level). For elite athletes, surgery will usually be performed after a shorter period of rehabilitation. Occasionally, ACL reconstruction surgery is required sooner than 4 to 6 weeks. This is especially when other ligaments on the outer side of the knee (posterolateral corner) are torn or when a displaced tear of the meniscus is locking the knee in one position.

Prior to undergoing surgery you will have further imaging of your knee to assess for associated injuries. The best test for this is an MRI scan which allows accurate assessment of damage to all the soft tissues around the knee such as other ligaments, cartilage and menisci. This will aid with the planning of your surgery and also allow us to provide you with more accurate information with regards to your likely rehabilitation program. Your rehabilitation after the operation is an important factor in the success of your surgery.
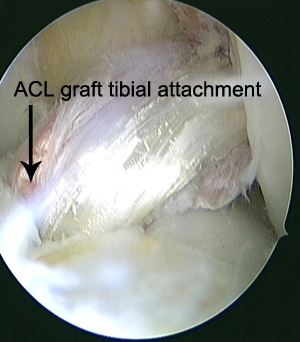
You will be admitted to hospital on the day of your surgery. Your anaesthetist will discuss with you the type of anaesthetic you will have and your options for post operative pain relief. Most patients have a regional anaesthetic. Antibiotics are delivered via a drip to decrease the risk of developing an infection. After your anaesthetic has been administered, a tight band (tourniquet) will be applied to your upper thigh and everything except your knee will be covered by sterile drapes. Two of your hamstring tendons (gracilis and semitendinosis) will be removed from the back of your thigh through an incision on the front of your knee. This is done with a special instrument called a tendon stripper. In some cases (eg. a revision operation), the knee cap ligament (the middle third of the patellar ligament) or the hamstring tendons from your opposite leg may need to be used. With the aid of a specialised telescope (arthroscope), the inside of your knee is inspected for any associated damage. If any is found (eg. a meniscal tear), it will be addressed at the time of surgery.A tunnel will be drilled in the top of your leg bone (tibia) and the bottom of your thigh bone (femur). The tendons will be passed through these tunnels and anchored in place with specialised devices (screws and buttons) to provide stability to your knee. Your knee will be injected with local anaesthetic to help with your post operative pain control. All your wounds will be closed using a combination of normal and dissolving sutures. Your leg will then be wrapped in a well-padded dressing prior to leaving the operating theatre.
A brace is usually applied after your surgery. You will be closely monitored until you are ready to return to your ward. An xray of your knee will be taken the day of your surgery. During your stay, you will be seen by a physiotherapist who will provide instructions for exercises for you leg that can be performed whilst in bed The aims of these visits are to regain motion in the knee, gradually improve your mobility, teach you exercises to maintain muscular strength around the knee and control your knee swelling.
You will be able take all your weight through the operated leg after the operation. Once you are mobilizing safely, have regained appropriate motion in the knee and your pain is controlled by oral pain medication you will be able to go home. The majority of patients are able to be discharged home the next day of their surgery
During the first week at home your knee will be swollen and feel stiff. It is normal to require regular pain medication during this period. It is of utmost importance that you perform your rehabilitation exercises regularly whilst at home so that you get the greatest possible benefit from your surgery. These exercises are given to you on an instruction sheet prior to your hospital discharge. Prior to discharge from hospital, a post operative visit to your surgeon will be organised approximately 10-14 days following your surgery.
Rehabilitation after an ACL reconstruction takes approximately 6 months. During this period you will take part in a structured rehabilitation program with your physiotherapist, and gradually return to your normal activities. This process is designed to safely improve the strength, motion and balance (proprioception) in your knee. You should follow-up with your surgeon at 2 and 6 weeks, then three, six and twelve months after your surgery.